


Overview
Tetralogy of Fallot (teh-TRAL-uh-jee of fuh-LOW) is a rare heart condition that is present at birth. That means it's a congenital heart defect. A baby born with Tetralogy of Fallot has four different heart conditions.
The four heart conditions affect the structure of the heart. As a result, there are changes in blood flow through the heart and to the rest of the body. Babies with tetralogy of Fallot often have blue or gray skin color due to low oxygen levels.
Tetralogy of Fallot is usually diagnosed during pregnancy or soon after a baby is born. If the heart changes and symptoms are mild, tetralogy of Fallot may not be noticed or diagnosed until adulthood.
Babies with tetralogy of Fallot need surgery to fix the heart. They also need regular health checkups for life.
Symptoms
Tetralogy of Fallot symptoms depend on how much blood flow is blocked from leaving the heart to go to the lungs. Symptoms may include:
- Blue or gray skin color. Depending on skin color, these changes may be harder or easier to see.
- Shortness of breath and rapid breathing, especially during feeding or exercise.
- Trouble gaining weight.
- Getting tired easily during play or exercise.
- Crankiness.
- Crying for long periods of time.
- Fainting.
Tet spells
Some babies with tetralogy of Fallot suddenly develop deep blue or gray skin, nails and lips. This usually happens when the baby cries, eats or is upset. These episodes are called tet spells.
Tet spells are caused by a rapid drop in the amount of oxygen in the blood. They are most common in young infants, around 2 to 4 months old. Tet spells may not be as easy to see in toddlers and older children. That's because toddlers and older children typically squat when they're short of breath. Squatting sends more blood to the lungs.
When to see a doctor
Serious congenital heart conditions such as tetralogy of Fallot are often diagnosed before or soon after a baby is born. Seek medical help if you notice that your baby has these symptoms:
- Trouble breathing.
- Blue or gray color of the skin.
- Lack of alertness.
- Seizures.
- Weakness.
- More cranky than usual.
If your baby's skin becomes blue or gray, place your baby on the side and pull the baby's knees up to the chest. This helps increase blood flow to the lungs. Call 911 or your local emergency number right away.
Causes
Tetralogy of Fallot happens during pregnancy when the baby's heart grows. Usually, the cause isn't known.
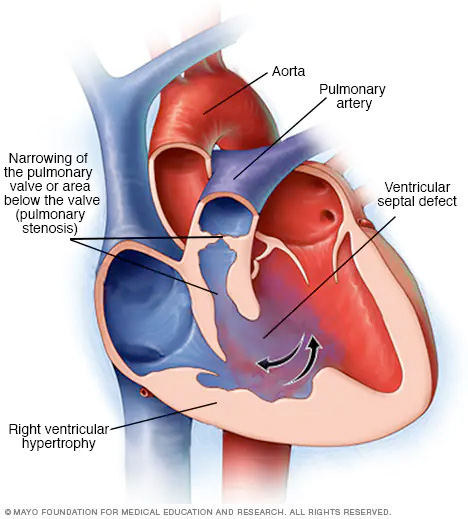
Tetralogy of Fallot includes four changes in heart structure:
- Narrowing of the valve between the heart and the lungs, called pulmonary valve stenosis. This condition reduces blood flow from the heart to the lungs. The narrowing may just involve the valve. Or it could happen in more than one place along the pathway between the heart and lungs. Sometimes the valve isn't formed. Instead, a solid sheet of tissue blocks blood flow from the right side of the heart. This is called pulmonary atresia.
- A hole between the bottom heart chambers, called a ventricular septal defect. A ventricular septal defect changes how blood flows through the heart and lungs. Oxygen-poor blood in the lower right chamber mixes with oxygen-rich blood in the lower left chamber. The heart has to work harder to pump blood through the body. The problem may weaken the heart over time.
- Shifting of the body's main artery. The body's main artery is called the aorta. It's usually attached to the left lower heart chamber. In tetralogy of Fallot, the aorta is in the wrong place. It's shifted to the right and sits directly above the hole in the heart wall. This changes how blood flows from the aorta to the lungs.
- Thickening of the right lower chamber of the heart, called right ventricular hypertrophy. When the heart has to work too hard, the wall of the right lower heart chamber gets thick. Over time, this may cause the heart to become weak and stop pumping blood as well as it should.
Some people with tetralogy of Fallot have other changes that affect the aorta or heart arteries. There also may be a hole between the heart's upper chambers, called atrial septal defect.
Risk factors
The exact cause of tetralogy of Fallot isn't known. Some things may raise the risk of a baby being born with tetralogy of Fallot. Risk factors include:
- Family history of the condition.
- Having a virus during pregnancy. This includes rubella, also known as German measles.
- Drinking alcohol during pregnancy.
- Eating poorly during pregnancy.
- Smoking during pregnancy.
- Being older than 35 during pregnancy.
- Down syndrome or DiGeorge syndrome in the baby.
Complications
Without treatment, tetralogy of Fallot usually leads to life-threatening complications. The complications may cause disability or death by early adulthood.
A possible complication of tetralogy of Fallot is infection of the inner lining of the heart or heart valves. This is called infective endocarditis. Sometimes medicines called antibiotics are given before dental work to prevent this type of infection. Ask your healthcare team if preventive antibiotics are right for you or your baby.
Complications also are possible after surgery to repair tetralogy of Fallot. But most people do well after such surgery. When complications occur, they may include:
- Backward flow of blood through a heart valve.
- Irregular heartbeats.
- A hole in the heart that doesn't go away after surgery.
- Changes in the size of the heart chambers.
- Swelling of part of the aorta, called aortic root dilation.
- Sudden cardiac death.
Another treatment or surgery may be needed to fix these complications.
Congenital heart defects and pregnancy
People born with a complex congenital heart defect may be at risk of complications during pregnancy. Talk with your healthcare team about the possible risks and complications of pregnancy. Together you can discuss and plan for any special care needed.
Prevention
Because the exact cause of most congenital heart defects isn't known, it may not be possible to prevent these conditions. If you have a high risk of giving birth to a child with a congenital heart defect, genetic testing and screening may be done during pregnancy.
There are some steps you can take to help lower your child's overall risk of birth defects, such as:
- Get proper prenatal care. Regular checkups with a healthcare team during pregnancy can help keep the pregnant parent and baby healthy.
- Take a multivitamin with folic acid. Taking 400 micrograms of folic acid daily can lower the risk of birth defects in the brain and spinal cord. It may help lower the risk of heart defects as well.
- Don't drink or smoke. These lifestyle habits can harm a baby's health. Also stay away from secondhand smoke.
- Get a rubella vaccine, also called a German measles vaccine. An infection with the rubella virus during pregnancy may affect a baby's heart development. Get vaccinated before trying to get pregnant.
- Manage blood sugar. If you have diabetes, managing your blood sugar can lower the risk of congenital heart defects.
- Manage long-term health conditions. If you have other health conditions, including a rare inherited condition called phenylketonuria, talk with your healthcare team. Ask about the best ways to treat and manage them.
- Stay away from harmful substances. During pregnancy, have someone else do any painting and cleaning with strong-smelling products.
- Check with your healthcare team before taking any medicines. Some medicines can cause birth defects. Tell your healthcare team about all the medicines you take, including those bought without a prescription.
Diagnosis
Tetralogy of Fallot is often diagnosed soon after birth. Your baby's skin may look blue or gray. A whooshing sound may be heard when listening to the baby's heart with a stethoscope. This is called a heart murmur.
Tests
Tests to diagnose tetralogy of Fallot include:
- Oxygen level measurement. A small sensor placed on a finger or toe quickly checks the amount of oxygen in the blood. This is called a pulse oximetry test.
- Echocardiogram. This test uses sound waves to create pictures of the heart in motion. It shows the heart and heart valves and how well they are working.
- Electrocardiogram. Also called ECG or EKG, this test shows how the heart is beating. Sticky patches called electrodes go on the chest and sometimes the arms or legs. Wires connect the patches to a computer. The computer prints or displays results. An electrocardiogram can help diagnose an irregular heartbeat. Changes in the heart signals also may be due to an enlarged heart.
- Chest X-ray. A chest X-ray shows the shape and condition of the heart and lungs. A common sign of tetralogy of Fallot on an X-ray is a boot-shaped heart. That means the right lower chamber is too big.
- Cardiac catheterization. This test helps diagnose or treat some heart conditions. It may be done to plan surgery. The doctor inserts one or more thin, flexible tubes into a blood vessel, usually in the groin. The tubes, called catheters, are guided to the heart. During the test, doctors can do different heart tests or treatments.
Treatment
All babies who have tetralogy of Fallot need treatment with surgery to fix the heart and improve blood flow. A heart surgeon, called a cardiovascular surgeon, does the surgery. The timing and type of surgery depends on the baby's overall health and specific heart changes.
Some babies or young children are given medicine while waiting for surgery to keep blood flowing from the heart to the lungs.
Surgery or other procedures
Surgery used to treat tetralogy of Fallot may include:
-
Temporary surgery, also called temporary repair. Some babies with tetralogy of Fallot need a surgery to improve blood flow to the lungs for the short term while waiting for open-heart surgery. This type of treatment is called palliative surgery. A surgeon places a tube called a shunt between a large artery that comes off from the aorta and the lung artery. The tube creates a new path for blood to go to the lungs. This surgery may be done if a baby is born early or if the lung arteries aren't fully developed.
The shunt is removed during open-heart surgery to treat tetralogy of Fallot.
-
Open-heart surgery, called complete repair. People with tetralogy of Fallot need open-heart surgery to completely fix the heart.
A complete repair usually is done in the first year of life. Rarely, a person may not have surgery in childhood if tetralogy of Fallot doesn't get diagnosed or if surgery is not available. Surgery still may help these adults.
A complete repair is done in several steps. The surgeon patches the hole between the lower heart chambers and repairs or replaces the pulmonary valve. The surgeon may remove thickened muscle below the pulmonary valve or widen the smaller lung arteries.
After complete repair, the right lower chamber doesn't need to work as hard to pump blood. As a result, the right chamber wall should go back to its usual thickness. The oxygen level in the blood goes up. Symptoms usually get better.
Outlook
The long-term survival rates for people who've had tetralogy of Fallot surgery continue to improve.
People with tetralogy of Fallot need lifelong care, ideally from a healthcare team that specializes in heart diseases. The health checkups often include imaging tests to see how well the heart is working. Tests also are done to check for surgery complications.
Lifestyle and home remedies
After treatment for tetralogy of Fallot, your healthcare team may suggest some steps to keep the heart healthy. These may include:
- Limits on sports and activity. Some people born with a serious heart condition such as tetralogy of Fallot may need to limit exercise or sports activities. But many others can take part in such activities. Ask your or your child's healthcare team which sports and types of activities are safe.
- Antibiotics to prevent heart infection. Sometimes, severe heart conditions can raise the risk of infection in the lining of the heart or heart valves. This infection is called endocarditis. Antibiotics may be recommended before dental treatments, especially for people who have a mechanical heart valve. Ask your or your child's healthcare professional if preventive antibiotics are needed. Good oral care and regular dental checkups also are important ways to help prevent infection.
Coping and support
You may find that talking with other people who've been in the same situation brings you comfort and encouragement. Ask your healthcare team if there are any support groups in your area.
Living with a congenital heart condition can make some people feel stressed or anxious. Talking with a therapist or counselor also may help you and your child learn new ways to manage stress and anxiety. Your care team can suggest therapists who may help you or your child.
Preparing for an appointment
Serious congenital heart defects such as tetralogy of Fallot typically are diagnosed during pregnancy or soon after birth.
If you think your child has a heart condition that wasn't noticed at birth, talk with your child's healthcare team. Be prepared to describe your child's symptoms. Ask family members if anyone was born with a heart condition, called a congenital heart defect. Some congenital heart defects may occur in families.
Here's some information to help you get ready for your appointment.
What you can do
If you have time to prepare for the medical visit, consider taking these steps.
- Make a list of your or your baby's symptoms, including any that don't seem related to tetralogy of Fallot.
- Write down your or your child's family history, including details from both sides of the family.
- Note any medicines, vitamins or other supplements taken during pregnancy if possible.
- Ask a family member or friend to come with you, if possible. Sometimes it can be hard to remember all of the information given to you during an appointment.
- Write down questions to ask the healthcare team.
For tetralogy of Fallot, some basic questions to ask your or your child's healthcare professional include:
- What's the most likely cause of this condition?
- Are there other possible causes of these symptoms?
- What kinds of tests do I or my child need? Do these tests require special preparation?
- What treatments are available, and which do you recommend?
- What are the possible complications of treatment?
- What is the outlook after surgery?
- Are there any activity restrictions?
- Can my child play sports or take part in gym class?
- Are there any brochures or other printed material that I can take home with me? What websites do you recommend?
Don't hesitate to ask other questions.
What to expect from your doctor
You'll usually be asked many questions, such as:
- When did you first notice your child's symptoms?
- Can you describe your child's symptoms?
- When do these symptoms occur?
- Do the symptoms come and go, or does your child always have them?
- Do the symptoms seem to be getting worse?
- Is there a family history of congenital heart defects?
- Does anything make your child's symptoms better?
- Has your child been growing and meeting developmental milestones as expected? Ask your child's healthcare professional if you're not sure.
© 1998-2026 Mayo Foundation for Medical Education and Research (MFMER). All rights reserved. Terms of Use